
Endocannabinoids in the Treatment of Prostate Cancer
An in-vitro study (i.e., outside of the body, e.g., studying individual cells under a microscope) published in Oncology Reports in January 2015 found that stimulation of cannabinoid receptors helped to stimulate apoptosis (i.e., programmed cell death) in prostate cancer cells.
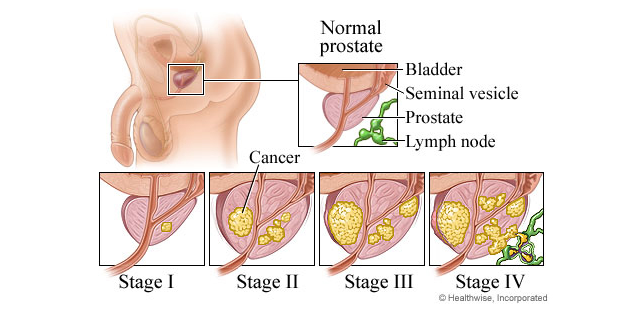
What is Prostate Cancer?
 Prostate cancer is caused by an overproliferation of abnormal cells of the prostate (a gland in the male body that secretes fluids that aid in reproduction). Tumors can press on or block surrounding structures or spaces, causing dysfunction in normal body processes, and in later stages cancerous cells can metastasize (i.e., invade distant organs), potentially causing extensive damage and, if uncontrolled, death.
Prostate cancer is caused by an overproliferation of abnormal cells of the prostate (a gland in the male body that secretes fluids that aid in reproduction). Tumors can press on or block surrounding structures or spaces, causing dysfunction in normal body processes, and in later stages cancerous cells can metastasize (i.e., invade distant organs), potentially causing extensive damage and, if uncontrolled, death.
Cancer of the prostate is the most common type of cancer found, and the second leading cause of cancer deaths, in males. In 2014, approximately 233,000 men in the United States were diagnosed with prostate cancer (14% of all cancer diagnoses), and approximately 29,480 men passed away as a result (5% of all cancer deaths).
When discovered early, there is a large chance that prostate cancer can be cured, with a 98.9% chance of surviving at least 5 years post-diagnosis. However, if the cancer is not detected until a later stage, by which time it may have metastasized, there is a much larger chance that it will lead to significant health problems and death. While there are treatment options for patients with late-stage, aggressive prostate cancer, they are less effective and fewer than those for patients with prostate cancer still in early stages.
According to the American Cancer Society, around the age of 50, most men should begin speaking with their physicians about when to begin screenings for prostate cancer. However, those with an increased risk of developing prostate cancer (e.g., black men or men with an immediate family member, such as a father or brother who developed prostate cancer before the age of 65) should begin speaking with their physicians about when to begin screening around the age of 45.
Past Evidence for Cannabinoids as Anti-Cancer Agents
Prior evidence found to support the potential for cannabinoids to work as anti-cancer agents, through the prevention of cancer cell formation and division, has shown their potential influence in:
- preventing stimulation of adenylate cyclase and protein kinase A, enzymes that lead to increased cell signaling that lead to increased growth, survival, etc.
- stopping the process by which cells divide by preventing production of inhibiting proteins, reducing the number of receptors and molecules that lead to increased cell growth (such as the epidermal growth factor, nerve growth factor receptors, and vascular endothelial growth factor and the hormone prolactin)
Additionally, the potential for cancer cells to invade local tissues and organs (which signifies a more aggressive cancer) is decreased by compounds that block receptors usually stimulated by endocannabinoids.
Results of the Study
Researchers treated/examined (1) prostate cancer cells (lines PC3 and PrC) and (2) cells from patients with benign prostatic hyperplasia (BPH, a condition that results in an increased number of prostate cells that are not cancerous):
- histologically (i.e., using a microscope): stained cells in order to visualize cannabinoid (CB1 and CB2) receptors, and
- by treating individual cells for (1) 48 hours with 2.5, 5.0 or 10 µM of either anandamide, 2-AG, or methanandamide (endocannabinoids, i.e., cannabinoids found naturally within the body) or (2) for 30 minutes with 10 or 20 µM of rimonabant (a CB1 receptor antagonist; an agent that prevents CB1 receptor stimulation) followed by treatment with the endocannabinoids.
Here is what they found:
- more CB1 and CB2 receptors found in aggressive prostate cancer cells than in less aggressive prostate cancer cells or BPH cells
- after treatment with endocannabinoids, cell survival was decreased in a statistically significant manner (i.e., in this case, there was a less than 5% chance that these results occurred merely by chance, rather than as a direct result of treatment)
- the higher the dose of endocannabinoid used, the greater the decrease in cell number (i.e., “dose dependence” was exhibited)- effect greatest for PC3 cells > BPH > PrC
- although expected among PC3, PrC, or BPH cells when treated with 5 µM of endocannabinoids, the cell’s growth cycle was not inhibited in comparison to those that were untreated (dose used may not have been high enough)
- when treated with 20 µM of the cannabinoid receptor antagonist, cell survival was not decreased– when treating the same cells with endocannabinoids, cell survival still was not decreased (likely as a result of the CB1 receptors being blocked)
- when 10 µM of cannabinoid receptor antagonist was used followed by treatment with cannabinoids, cell survival then began to decrease in PC3 cells (i.e. not enough CB1 receptors were blocked by the antagonist in order to prevent the protective effects of the endocannabinoids)
- between PC3 than in PrC cells, number of cells going through programmed-cell death was higher in cell lines treated with endocannabinoids than in those not being treated with endocannabinoids, with a stronger effect for PC3 cells
- between PrC and BPH cells, after 48-treatment with 5 µM of endocannabinoids, there was an increase in caspase-3 (enzyme that helps to activate programmed cell death) and a decrease in Bcl-2 (a protein that helps to prevent programmed cell death)
- in PrC cells, after 48-treatment with 5 µM of endocannabinoids, there were modifications in cell signaling pathways whose over-activation is commonly associated with cancer formation and propagation- increased activity in Erk pathway, decreased activity in Akt pathway
The authors note, “These results suggest that the effect of endocannabinoids on [prostate cancer] cells… may be caused by the activation of the apoptotic pathway… The great advantage that the use of endocannabinoids may bring to the battle against prostate cancer is that it has been demonstrated that the receptors for these molecules are substantially overexpressed in cancerous prostatic cells when compared to normal, healthy prostate tissues… Based on these results, we suggest that endocannabinoids may be a beneficial option for the treatment of prostate cancer that has become nonresponsive to common therapies.”
Symptom Relief
Individuals with prostate cancer who are finding it difficult to control certain symptoms that may be experienced as a result of the disease or treatment with standard therapies (such as pain, cachexia [“wasting syndrome”], anorexia [the symptom, not the disorder “anorexia nervosa”], nausea, and vomiting) may experience some relief through the use of whole-plant cannabis or the approved cannabinoid medication like dronabinol (i.e., synthetic THC; treatment with dronabinol has sometimes been associated with high levels of anxiety in patients due to the absence of other cannabinoids to dull the impact of the psychoactive effects of THC). Whole-plant cannabis use should be carefully discussed with and monitored by a healthcare professional, and individuals using whole-plant cannabis should not expect that use will prevent or treat prostate cancer.
Conclusion
In whole-plant or isolated forms, cannabinoid therapies have the potential to not only control symptoms caused by the disease and its treatment, but also potentially to inhibit its progression.
Given (1) these and past results, (2) that late-stage prostate cancer patients have limited treatment options, and (3) that cannabinoid therapies have a favorable side effect profile, their use is relatively safe as a potential additional experimental therapy for individuals with late-stage prostate cancer. Further research is needed in order to determine whether or not cannabinoid therapies will prove clinically useful as a reasonable and effective option for the prevention or treatment of prostate cancer in humans.
Before beginning whole-plant cannabis use, individuals with prostate cancer should consult with and have any possible use monitored by a healthcare provider; therefore, suitable recommendations can be given, and benefits or harmful side effects can carefully monitored and addressed when necessary.
For information on reasonable expectations and safety in considering whole-plant medical cannabis use, as well as how you can advocate to move cannabis out of the Schedule I controlled substance classification in order to increase research on phytocannabinoids in the United States, click here.