
The Accepted Medical Use of Marijuana: States Need To Take Action Now To Protect Patient Rights
After the recent rejection of the Rhode Island-Washington Marijuana Rescheduling Petition, it is easy to point fingers at the Drug Enforcement Administration (DEA) and proclaim how corrupt and inept they must be to uphold the position that marijuana still has no medical use. [1][2][3] However, once we see that the DEA and the Food and Drug Administration (FDA) both believe that the only way a drug substance can have medical use is for it to pass through the FDA’s own drug approval process, it’s easy to understand how the DEA is incapable of acknowledging a type of accepted medical use that it has no authority over.
The key to making sense of the DEA’s position regarding the medical use of marijuana is realizing that there are at least three types of accepted medical use.
The first, and most well known form of accepted medical use, results from successful completion of the FDA’s randomized placebo-controlled phase I-III clinical trials new drug approval process, which allows for an approved drug product to be marketed for interstate commercial distribution and carried by pharmacies as a prescription medication.
“[…] in Gonzales v. Oregon (2006), the Supreme Court confirmed the state’s right to accept the medical use of controlled substances by finding that the DEA does not have the authority to deny a standard of medical care that is accepted under state law.”
The second, and less obvious form of accepted medical use – known as “grandfathered” medical use – pertains to drugs that have been in widespread medical use prior to the adoption of the Food, Drug and Cosmetic Act of 1938. [4] Aspirin is the most prominent example of grandfathered medical use, as the over-the-counter formulation of this medication has never received FDA approval. [5]
The third, and least recognized form of accepted medical use, state-accepted medical use, exists because of the sovereign rights of individuals and our resulting form of government known as federalism, in which certain rights are retained by the states and others transferred by Congress to the federal government. The relevant example here is the authority of the state to accept the medical use of controlled substances, which falls under the state’s authority to regulate the profession of medicine within its own borders.
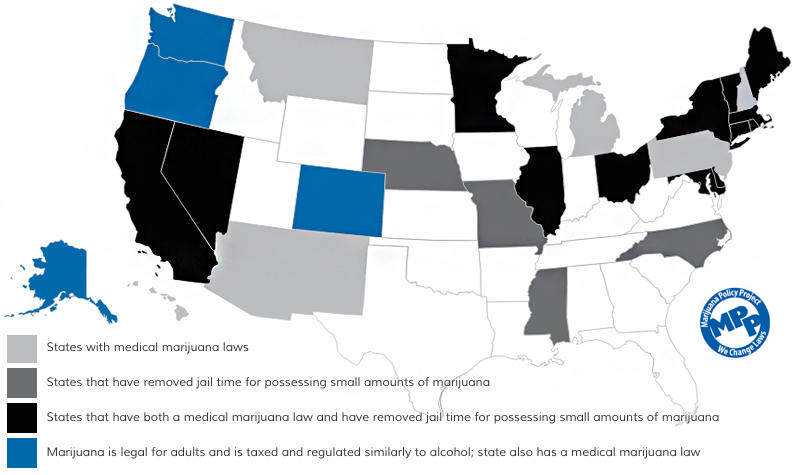
This authority has never been transferred to the federal government and is why more than half the states in the Union have been able to accept the medical use of marijuana and establish their own state-regulated Medical Use of Marijuana Programs, without legal challenge from the U.S. Department of Justice (DOJ). In fact, in Gonzales v. Oregon (2006), the Supreme Court confirmed the state’s right to accept the medical use of controlled substances by finding that the DEA does not have the authority to deny a standard of medical care that is accepted under state law. [6]
This is especially significant when such state-accepted medical use involves a Schedule I controlled substance, as in the case of cannabis, since such accepted medical use has a direct impact upon federal scheduling, a consequence that Congress was well aware of when it created the federal Controlled Substances Act in 1970 and provided a mechanism for states to affect changes in federal scheduling by means of the term “currently accepted medical use in treatment in the United States.” [7]
The Rhode Island-Washington Marijuana Rescheduling Petition failed because the governors of those states relinquished their state’s authority to accept the medical use of marijuana. By requesting a specific schedule change based on a scientific argument, they merely gave the DEA another chance to break out the 5-part test of “medical use” that it solely created in 1994 after two prior attempts at defining such use, and before any state had accepted the medical use of marijuana. [8][9][10][11]
Think of it this way, a landlord asks a tenant who is in default if he is going to honor the agreement they entered into wherein the tenant agreed to pay a set rent each month. Such an approach would most likely be fruitless. The landlord would be better served by giving the tenant notice that rent is due, and then pursuing court action if the tenant continues to ignore the agreement. Similarly, those states that have accepted the medical use of marijuana should give the DEA notice that marijuana has accepted medical use and needs to be removed from federal Schedule I.
 We need to approach this as a matter of law, not science. Given the DEA’s continued inaction regarding the medical use of marijuana, one solution for the current situation is for those states that have accepted the medical use of this substance to first make sure that marijuana is properly placed in a state schedule that recognizes its state-accepted medical use; and then give notice to the DEA that marijuana has accepted medical use and that its placement in federal Schedule I no longer applies. Such action by the states would demonstrate that they are doing their part to protect their state’s accepted medical use of marijuana, so that ultimately patients can be properly served and no longer placed in jeopardy by the violation of federal law.
We need to approach this as a matter of law, not science. Given the DEA’s continued inaction regarding the medical use of marijuana, one solution for the current situation is for those states that have accepted the medical use of this substance to first make sure that marijuana is properly placed in a state schedule that recognizes its state-accepted medical use; and then give notice to the DEA that marijuana has accepted medical use and that its placement in federal Schedule I no longer applies. Such action by the states would demonstrate that they are doing their part to protect their state’s accepted medical use of marijuana, so that ultimately patients can be properly served and no longer placed in jeopardy by the violation of federal law.
To make this happen everyone needs to get involved — contact your state legislators and executive officials to take action.
Citations & References
There are 11 references in this article. Click here to view them all.
- DEA Rejects Attempt to Loosen Federal Restrictions on Marijuana, NPR, August 10, 2016. http://www.npr.org/2016/08/10/489509471/dea-rejects-attempt-to-loosen-federal-restrictions-on-marijuana
- Denial of Petition to Initiate Rescheduling Proceedings for Marijuana, Federal Register, Vol. 81, No. 156, August 12, 2016, 53688. https://www.gpo.gov/fdsys/pkg/FR-2016-08-12/pdf/2016-17954.pdf
- DEA letter to Governors of Rhode Island and Washington, August 11, 2016. https://www.dea.gov/divisions/hq/2016/Letter081116.pdf
- History of the Food and Drug Administration, Wikipedia. https://en.wikipedia.org/wiki/History_of_the_Food_and_Drug_Administration
- Aspirin and Arthritis Go Together, But at What Risk ? http://www.arthritis-relief-naturally.com/aspirin.html
- Gonzales v. Oregon, 546 U.S. 243 (2006). https://www.law.cornell.edu/supct/html/04-623.ZS.html
- 21 USC 812: Schedules of Controlled Substances. https://www.deadiversion.usdoj.gov/21cfr/21usc/812.htm
- Rhode Island-Washington Marijuana Rescheduling Petition, November 30, 2011. http://files.iowamedicalmarijuana.org/imm/states/wa_federal_scheduling_20111130.pdf
- Grinspoon v. DEA (1st Cir. 1987). http://www.iowamedicalmarijuana.org/documents/grinspoon.aspx
- ACT v. DEA (D.C. Cir 1991). http://www.iowamedicalmarijuana.org/documents/act1.aspx
- ACT v. DEA (D.C. Cir. 1994). http://www.iowamedicalmarijuana.org/documents/act2.aspx